So what does a care plan include?
Care plans are one of the most used documents in adult social care. They are also one of the most poorly understood.
Many care workers encounter care plans on their first shift and are expected to read, follow, and contribute to them with very little formal guidance on what they should actually contain. Training often covers the principles of person-centred care. It covers the importance of documentation. What it rarely covers in detail is the specific content a care plan must include to be accurate, legally compliant, and practically useful.
That gap has consequences.
An incomplete care plan leaves the next care worker without the information they need. A generic care plan fails the person it is supposed to serve. An outdated care plan creates risk, not protection.
The Care Quality Commission identifies clear, current, and person-centred care plans as one of the strongest indicators of a safe and effective service. That means what a care plan includes is not a back-office question. It is a frontline one. It affects every shift, every handover, and every inspection.
This article sets out exactly what a care plan should include, why each section matters, and how structured training builds the confidence to do it well.
Quick Answer
A care plan is a written document that sets out exactly how a person’s health, well-being, and daily needs will be supported. It is person-centred, meaning it reflects the individual’s own wishes, routines, and goals rather than a generic checklist. In UK adult social care, care plans are both a legal requirement and the foundation of safe practice.
Table of Contents
What Is a Care Plan?
A care plan is a documented agreement between a care provider and the person receiving care. It describes what support is needed, how that support will be delivered, and who is responsible for each aspect of care.
Care plans are not just paperwork. They are working tools that guide every interaction between a care worker and the person they support. A well-written care plan means anyone stepping in for the first time knows exactly what to do, how to do it, and what matters most to the individual.
Why Care Plans Matter in the UK: The Data Behind the Duty
Understanding what a care plan includes becomes more urgent when you look at the scale of adult social care in England.
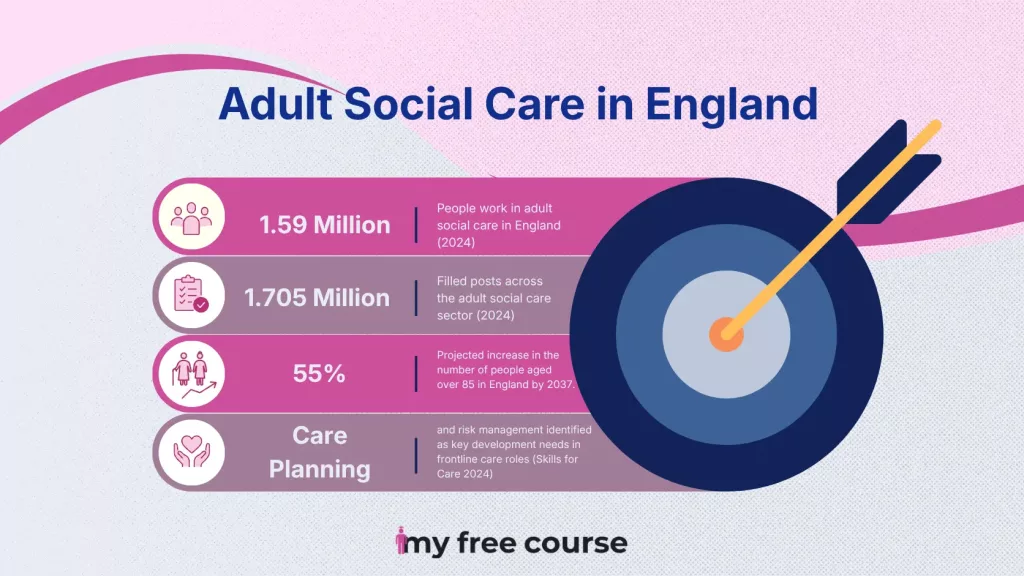
According to Skills for Care’s State of the Adult Social Care Sector and Workforce in England 2024, around 1.59 million people work in adult social care in England, with 1.705 million filled posts across the sector. National Health Service (NHS) planning documents project that the number of people aged over 85 in England will increase sharply over the next decade, rising by 55% by 2037.
With more people needing care, the quality and consistency of care planning become more critical every year. Skills for Care’s 2024 workforce data identifies care planning and risk management as key development needs in frontline care roles. Ongoing vacancy pressures make consistent care planning harder, particularly when staff have limited formal training.
Every care plan that is incomplete, outdated, or too vague to act on represents a gap in the safety net that care workers provide. Structured training helps workers produce clearer plans, maintain better records, and feel more confident during handovers and inspections.
What Does a Care Plan Include?
A thorough care plan covers multiple areas of a person’s life. The exact content varies depending on individual needs, but the following sections are standard across most adult social care settings in England.
Personal Information
Every care plan starts with essential identifying information. This includes the person’s full name, date of birth, address, NHS number, GP details, emergency contacts, and key professionals involved in their care.
This section ensures that anyone working with the individual, even for the first time, has all critical information in one place. It supports continuity of care across shift handovers, multi-agency working, and emergency situations.
If this section is incomplete or out of date, the entire care plan becomes less reliable in the moments when it matters most.
Assessed Needs and Goals
This is the central section of what a care plan includes. It describes what the person needs support with across areas, including personal care, mobility, nutrition, medication management, mental health, and social participation.
Goals are also recorded here. A goal might be to maintain independence with washing for as long as possible, or to attend a weekly social activity. Recording goals makes care active and forward-looking rather than simply reactive.
Under the Care Act 2014, care providers are legally required to promote the well-being, independence, and involvement of the people they support. This section is where that duty becomes visible in practice.
Support Actions and Responsibilities
For each identified need, the care plan documents exactly what support will be provided and how. This includes what the care worker will do, what the person will do for themselves, and what other professionals are involved.
Specificity is one of the most important qualities in a care plan. It is also one of the most commonly missing. A phrase like “provide personal care as needed” gives the next care worker no practical guidance. Every action should be specific enough that a new team member could follow it without needing to ask.
Risk Assessment
Every care plan must include identified risks and how they will be managed. Common areas include falls risk, skin integrity, choking and nutrition risk, self-neglect, and safeguarding concerns.
Skills for Care’s 2024 workforce data identifies risk management as one of the most significant skills gaps among frontline care workers. A well-structured risk assessment embedded in the care plan reduces incidents, protects the individual, and protects the care worker.
Risk assessments must be reviewed and updated. A risk assessment completed at the point of admission and never revisited does not reflect the person’s changing needs. It does not protect anyone.
Communication Preferences and What Matters to the Person
This section captures how the person prefers to communicate and what matters to them day to day. It covers language preferences, sensory needs, communication aids, daily routines, food preferences, cultural needs, and personal values.
This is the section that makes what a care plan includes genuinely person-centred rather than just procedurally complete. It is also, according to CQC inspection records, the most frequently under-completed section.
A person who cannot communicate verbally still has preferences, rhythms, and things that bring comfort. This section is where those things are recorded, so they are never forgotten during a handover.
Review Dates and Signatures
Care plans must be reviewed regularly to remain accurate and legally valid. The care plan records when it was last reviewed, who was involved in that review, and when the next review is due.
Most settings require a minimum annual review. Reviews should also take place immediately after any significant change in the person’s health, circumstances, or wishes. A care plan that is six months out of date after a hospitalisation is a care plan that cannot be trusted.
Signatures from both the care provider and, wherever possible, the person receiving care confirm that the plan reflects a shared agreement rather than a unilateral decision.
Sample of a Care Plan
To see how these sections work together in practice, consider Margaret, 82, living in a residential care home after a fall at home. Her care plan opens with her personal details, NHS number, GP contact, and her daughter listed as next of kin. Her assessed needs cover morning personal care assistance and moderate falls risk. Her goal, one she chose herself, is to walk to the communal garden independently by the end of the month. That detail matters. It makes the plan active rather than passive.
Her support actions are specific. A care worker assists with a seated wash and dressing between 7:30 and 8:30 each morning, while Margaret chooses her own clothing. Her risk assessment flags light-headedness from blood pressure medication. Her communication preferences note that she is hard of hearing on her left side, prefers Margaret over Maggie, and finds classical music calming during personal care.
Every section connects to the next. Together, they create a document that any care worker can follow with confidence on their first shift, while still seeing Margaret as a person rather than a list of tasks. That is what a good care plan is supposed to do.
Who Writes a Care Plan?
Care plans are usually initiated by a care manager or senior care worker following a formal needs assessment. However, updating and maintaining them is a shared responsibility across the care team.
The person receiving care must be involved in writing their own care plan. Under the Care Act 2014, this is not a best practice recommendation. It is a legal requirement. The individual’s voice must be present in every section of a plan that exists to serve them.
Family members and other advocates may also be involved, particularly where the person has limited capacity or communication difficulties. Multi-disciplinary input from GPs, occupational therapists, and district nurses is standard in complex cases.
Understanding what a care plan includes helps every member of the team contribute accurately and consistently, regardless of seniority.
Common Mistakes in Care Planning
Knowing what does a care plan include also means knowing what goes wrong and why. The following mistakes appear regularly in CQC inspection findings and in day-to-day care practice.
- Using vague or generic language: Phrases like “provide personal care as needed” give the next care worker no practical guidance. Every action should be specific enough that a new team member could follow it without needing to ask.
- Failing to update after a change: If a person’s mobility deteriorates or their medication changes, the care plan must be updated immediately. Not at the next scheduled review. Immediately.
- Not involving the person: A care plan completed without meaningful input from the individual is not legally compliant under the Care Act 2014 and is not person-centred in any meaningful sense.
- Treating risk assessment as a one-off exercise: Risk assessments completed once and never revisited do not protect anyone. They create a false sense of safety while leaving real risks unmanaged.
- Copying and pasting between care plans: Every person is different. A template is a starting point, not a finished document. Generic care plans are one of the clearest signals of institutional, rather than person-centred, care.
Care Plans and CQC Compliance
The CQC uses care plans as primary evidence when assessing whether a service is Safe, Effective, Caring, Responsive, and Well-Led across all five inspection areas.
The 2023/24 State of Care report noted that services which invest in care planning training consistently achieve stronger outcomes across all inspection domains. Inadequate or outdated care plans are cited as contributing factors in a significant proportion of enforcement actions and rating downgrades.
For care home owners and HR managers, care planning is directly connected to inspection outcomes. A workforce that understands care planning principles and can demonstrate that understanding to an inspector is one of the clearest indicators of a well-led service.
Funded training through the Adult Skills Fund means your team can access accredited care planning qualifications at no tuition cost. This removes the most common barrier to keeping knowledge current and documentation standards high.
How Training Improves Care Planning
Knowing what does a care plan include in theory is important. A nationally recognised qualification that demonstrates and develops that knowledge is what makes the difference in practice, in inspections, and in career progression.
Formal training gives care workers the frameworks, language, and confidence to write care plans that are specific, person-centred, and legally sound. It removes the uncertainty that comes from learning only on the job.
This course covers how to assess individual needs in a person-centred way, how to involve the person in decisions about their own care, how to document clearly and specifically, and how to manage personal care needs including nutrition, hygiene, and continence care.
It is fully online, self-paced, and assessed through coursework rather than formal exams. Tuition is funded through the Adult Skills Fund for eligible learners. Some partner colleges may charge an admin fee of £50 to £100.
This course is directly relevant to any care worker who writes, contributes to, or uses care plans in their daily role.
Frequently Asked Questions (FAQ)
What does a care plan include in adult social care?
A care plan typically includes personal information, assessed needs and goals, support actions and responsibilities, a risk assessment, communication preferences, and review dates. Each section should be specific, current, and written with the involvement of the person receiving care.
How often does a care plan need to be reviewed?
Care plans must be reviewed at a minimum of once per year. They should also be reviewed immediately following any significant change in the person’s health, circumstances, medication, or wishes. An out-of-date care plan is not a safe one.
What happens if a care plan is not followed?
Failing to follow a care plan can constitute a safeguarding failure, particularly if the person is harmed as a result. It can lead to CQC enforcement action, disciplinary procedures, and in serious cases, referral to a regulatory body.
What is the difference between a care plan and a support plan?
The terms are often used interchangeably. A care plan is the more common term in registered care settings. A support plan is more common in social work and supported living contexts. Both documents serve the same purpose: recording an individual’s needs and how those needs will be met.
Does a care plan have to be in writing?
Yes. In registered care settings in England, written care plans are a legal and regulatory requirement. Verbal agreements are not sufficient and would not meet CQC standards.
Is there funded training on what does a care plan include?
Yes. The Level 2 Certificate in the Principles of Care Planning is available through the Adult Skills Fund for eligible learners. Tuition is fully funded. Some partner colleges charge an admin fee of £50 to £100. Check eligibility here
Check Your Eligibility